


Shin and malleoli trauma
Fracture of shin proximal partEvulsion, compression, T and V-like fractures are marked among fractures of shin bone condyles. These traumas are often accompanied with damage of knee joint meniscus and ligaments and fractures of intracondylar elevation. Most of them are intraarticular and are usually accompanied with hemarthrosis. Hemarthrosis (hemorrhage into joint cavity) manifests in severe edema and needs punction with following extraction of blood. Shin bone condyle fracture with no dislocation needs immobilization with back plaster splint with sole fixation and limitation of loads on the leg for 2 – 3 months. In cases of dislocation the main condition of treatment an ideal reposition of articular surface and shin bone axe preservation is. Reposition performed is opened – with osteosynthesis or closed one – under arthroscopic control. 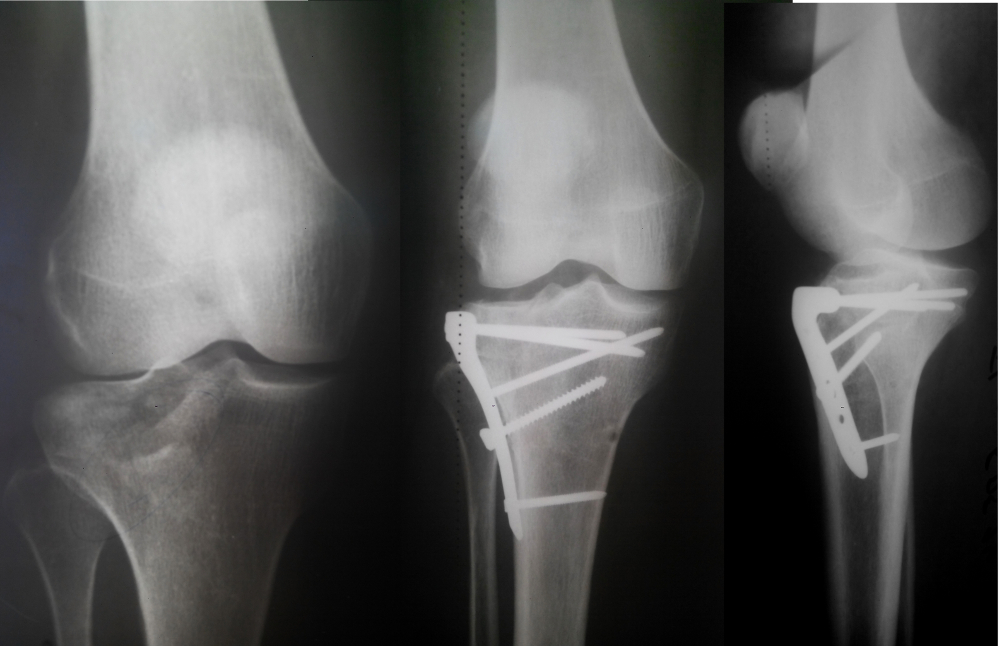 Tibia and fibula diaphysis fracturesFractures of shin bone mid third are divided into transversal, oblique, screw-like and fragmental ones. Direct mechanism of trauma more often leads in transversal and fragmental fractures. Torsion and flexion cause screw-like and oblique fractures. Diagnostics of shin bone mid third fractures is not complicated even for not medically educated person. Intramedular osteosynthesis is the most common method of treatment of these fractures. On the boundary of middle and lower thirds of a shin bone there is a zone lack in blood supply and nonunion tendency. Treatment of such fracture requires less invasiveness and blood circulation preservation. In tibia osteosynthesis fibula is synthesized in its lower third fracture only. In these cases its axe may influence the ankle biomechanics. 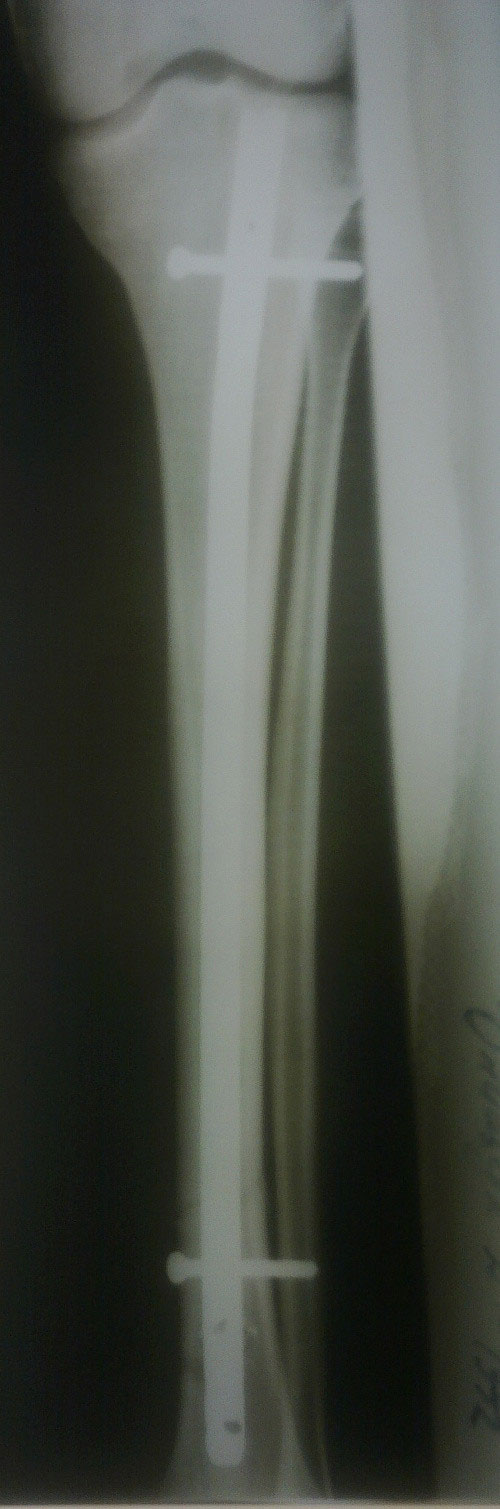 Malleoli fractureThis fracture is the most common one among fractures of a lower limb and more often occurs in time. Is caused by rotation mechanism and may be pronation and supination one. Almost all malleoli fractures are treated operatively as far as almost all of them tend to dislocate. Malleoli are small parts of a shin bones forming an ankle. Ankle has the organism greatest load and therefore an articular surface requires an ideal approximation of fragments. If malleoli fracture is accompanied with an intratibial articulation damage, it is synthesized with positional screw or screw-strainer. The load is permitted 1 – 2 months after an intervention.  Patella fractureMusculus quadriceps femoris extending shin bone through patella proper ligament is jointed to patella. This explains patient’s inability to rise his leg in patella fracture. In transversal fractures it is possible to palpate two poles of patella. Immobilization may be used in case of fractures with no dislocation. Patella complete fracture with dislocation and musculus quadriceps femoris ligament damage should be treated operatively. Tibia extending apparatus provides walking function, therefore traumas of these structures require restoration of patella articular surface and ligaments length.
Achilles tendon damageAchilles tendon (calcaneal, heel tendon) – is the strongest in our organism as it takes a whole body weight in each step of a human. The main symptoms of its damage is inability to stand on the anterior part od a sole and pain across posterior surface of an ankle. Complete rupture of heel tendon is sutured with huge bioabsorbed threads which are resolving. Treating of this trauma requires essential immobilization even after an operative intervention. The bandage has a psychological effect as well and helps the patient to remember about limitation of loads in knitting period. |
